

Background:
Clinical trials are the gold standard by which therapies in oncology are evaluated and ultimately form the bases for approval of novel therapies. Stringent eligibility criteria limit the participation of many "real-world" patients and thus undermine the generalizability of trial results. Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of Non-Hodgkin lymphoma (NHL) and is curable in the majority of patients treated with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). The addition of rituximab to CHOP is the only clear advancement in DLBCL therapy in the last 20 years. Though a large minority of patients are not cured by R-CHOP, several subsequent novel therapies have failed to demonstrate benefit in Phase 3 clinical trials. We hypothesized that real world patient populations differ from clinical trial populations with trial eligibility excluding the poor-outcome patients who might benefit most from novel therapy.
Methods:
We performed a retrospective chart review of all patients 18 years of age or older who were registered within the Alberta Cancer Registry with a new diagnosis of pathology-confirmed DLBCL, between January 1, 2010 and December 31, 2011. Clinical characteristics were reviewed to assess patient eligibility to participate in 3 landmark clinical trials for DLBCL on the basis of inclusion and exclusion criteria defined by each study. The trials included Pfreundschuh, M. et al. (2006) and Coiffier, B. et al. (2002), which were assessed together as representing the landmark studies for rituximab added to CHOP, and the GOYA trial (2017) which evaluated obinutuzumab-CHOP vs R-CHOP. Categorical variables are presented as frequencies and percentages. Univariate probabilities of overall-survival were calculated by Kaplan-Meier method.
Results:
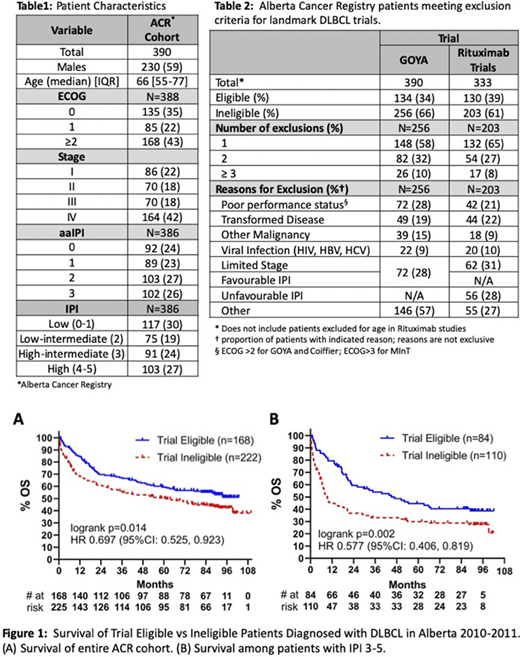
We identified 480 patients with a diagnosis of DLBCL within the Alberta Cancer Registry. A total of 390 patients were eligible for our study with 20 patients excluded for CNS lymphoma, 29 for unclassifiable B-cell lymphoma, 2 patients who died at the time of diagnosis, and 25 patients with previously treated indolent lymphoma. In addition, 14 patients were excluded for insufficient clinical data. Table 1 demonstrates the clinical characteristics of the population. Out of 390 patients, only 130 (33%) patients met inclusion for the rituximab studies and 134 (34%) for the GOYA study. Table 2 demonstrates the most common criteria leading to trial exclusion, including poor performance status, limited stage disease, inappropriate IPI, transformed lymphoma, history of second primary malignancy, and viral infections. Trial ineligible patients had significantly inferior overall survival compared to trial eligible patients (Figure1).
Conclusions:
The majority of real-world DLBCL patients are excluded from clinical trials and have inferior outcomes compared to trial eligible patients. The selection of patients with more favourable outcomes for clinical trials may contribute to failure to demonstrate a benefit of novel therapies. Broadening inclusion criteria to include patients with transformed disease and poor performance status could aid in improving the generalisability of DLBCL clinical trials.
Stewart:Gilead: Honoraria; Roche: Honoraria; Celgene: Honoraria; Amgen: Honoraria; Abbvie: Honoraria; Janssen: Honoraria; Teva: Honoraria; Sandoz: Honoraria; AstraZeneca: Honoraria; Novartis: Honoraria. Owen:AbbVie, F. Hoffmann-La Roche, Janssen, Astrazeneca, Merck, Servier, Novartis, Teva: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal